A kidney infection can become life-threatening within hours to a few days if it progresses to sepsis and septic shock, especially in high-risk individuals or when treatment is delayed, though prompt antibiotics usually prevent fatal outcomes and most people recover. The average time to death in modern urosepsis cohorts is on the order of days after diagnosis (mean around 8 days), underscoring that early recognition and rapid treatment are critical to avoid the rare but real risk of mortality.
Table of Contents
What does “how fast can a kidney infection kill you” mean
The question “how fast can a kidney infection kill you” is really about the speed at which pyelonephritis can escalate into urosepsis and septic shock, which can be fatal without timely care. While most kidney infections respond quickly to antibiotics, severe cases can deteriorate rapidly—sometimes within 24–72 hours—if the infection spreads to the bloodstream and overwhelms the body’s response, particularly in older adults or those with comorbidities. This dual reality—generally good outcomes but potential for swift decline—explains why urgent evaluation and treatment are emphasized in medical guidance.
How fast can it turn deadly?
- Progression to sepsis can occur within 24–48 hours after severe symptom onset if care is delayed, based on specialty urology guidance summaries and clinical overviews.
- Authoritative health systems note life-threatening complications (sepsis, septic shock, organ failure) can follow kidney infections, particularly in vulnerable groups or when undertreated.
- In a multicenter European cohort of confirmed urosepsis, mean time to death from diagnosis was 8.4 days (range 3.6–25.2), indicating that once sepsis is established, the fatal window spans days, not weeks, and that early in-hospital management is crucial.
Typical trajectory and red flags
- Kidney infections often begin with fever, flank pain, and urinary symptoms; worsening to high fever, chills, vomiting, confusion, low blood pressure, or rapid breathing suggests sepsis and demands immediate emergency care.
- Health sources stress that untreated kidney failure from severe infection could lead to death within days to weeks, and that bloodstream spread (urosepsis) is a medical emergency requiring rapid antibiotics and often source control (e.g., relieving obstruction).
- Rapid deterioration is more likely with age >65, diabetes, obstruction (e.g., stones), indwelling catheters, pregnancy, or immunosuppression, so thresholds for urgent assessment should be low in these populations.
Evidence at a glance
- A prospective multicenter study (SERPENS) of 354 urosepsis patients found 30‑day mortality 2.8% overall, 4.6% in severe sepsis, with all deaths occurring among those presenting with organ failure (SOFA ≥2).
- The same study reported most patients recovered by day 30 (73.1%), but 24.0% still had organ failure, and initial multi-organ failure fell from 48% at baseline to 7% at day 30, illustrating both reversibility and risk.
- Large observational work on complicated pyelonephritis shows severe sepsis/septic shock at admission in about 28%, with markedly higher 30-day mortality in those severe groups (crude 17.7% vs 1.7%).
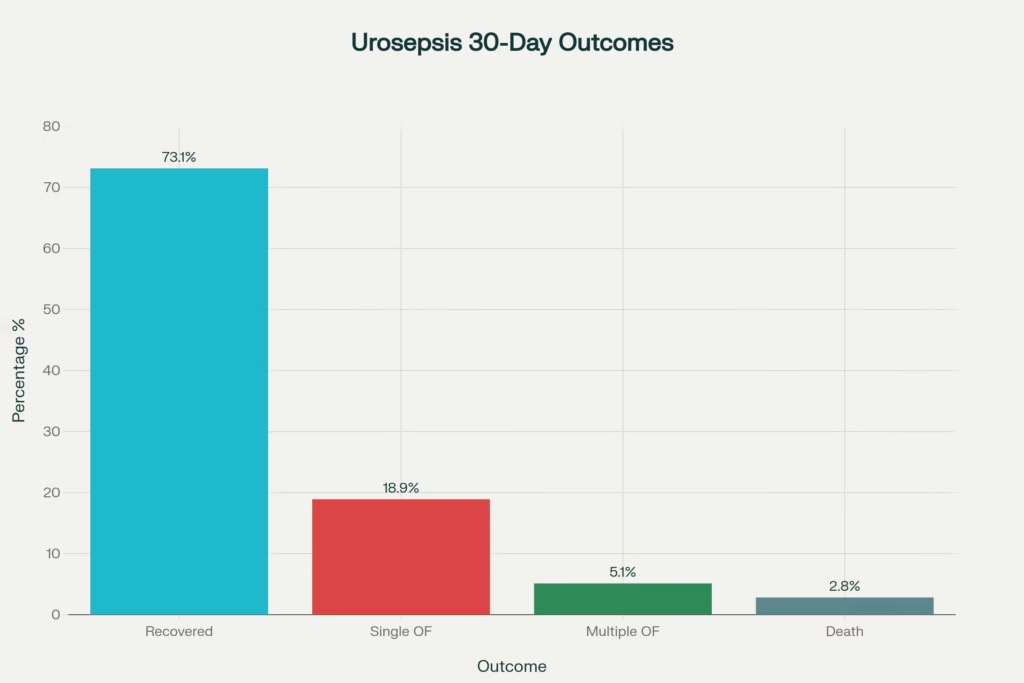
Distribution of 30-day outcomes in urosepsis from the SERPENS study
Who is at highest risk
- Older adults (especially >65 years), people with diabetes, pregnant patients, immunocompromised individuals, those with urinary obstruction or stones, recent urinary instrumentation, or indwelling catheters face faster escalation and worse outcomes.
- In the SERPENS cohort, risk of organ failure and death rose with higher Charlson comorbidity index, baseline respiratory failure, recent ICU admission, urinary obstruction, MDR pathogens, and SOFA ≥2 at diagnosis.
- These findings mirror emergency department observations that bacteremia, lack of classic symptoms, and significant hydronephrosis/ectasia are tied to severe sepsis risk in complicated cases.
How “fast” in real life scenarios
- Early sepsis: Hours to 1–2 days after severe symptoms in susceptible patients or when treatment is delayed, per clinical overviews and urology guidance.
- Deterioration window: After diagnosis of urosepsis, deaths occurred over days (mean ~8.4 days), indicating a brief period to reverse organ failure with aggressive management.
- Without treatment: Health resources warn that kidney failure from severe infections can be fatal within days to weeks, but this scenario is largely preventable with timely care.
Treatment speed matters
- Time to antibiotics is a defining factor; in the SERPENS study, median time from diagnosis to first antibiotic dose was 60 minutes, with high appropriateness (89% susceptibility match) and urgent relief of obstruction in many cases—practices aligned with improved outcomes.
- Guidelines and health system pages emphasize seeking immediate care for pyelonephritis symptoms; most people feel better within 2–3 days of starting appropriate antibiotics, though completing the full course is essential to avoid relapse or complications.
- When needed, hospital care includes IV antibiotics, fluids, vasopressors, and procedures to relieve blockage (stents/nephrostomy), which can quickly reverse hemodynamic instability and improve survival.
Statistics to know
- Annual incidence: Kidney infection affects roughly 1 in 2,000 people per year in the U.S., underscoring relative rarity compared to lower UTIs but higher severity.
- Urosepsis burden: UTIs account for an estimated 20–40% of all sepsis cases, making urinary sources a common sepsis origin worldwide.
- Mortality gradients: Overall urosepsis 30‑day mortality ~2.8% in the SERPENS study, increasing to ~4.6% in severe sepsis, and much higher in severe sepsis/septic shock cohorts of complicated pyelonephritis in other series.
Case studies and exemplars
- Emphysematous pyelonephritis (EPN): A severe, gas-forming kidney infection often in uncontrolled diabetes; case reports show patients presenting with sepsis who improve with early broad-spectrum antibiotics and supportive care, although EPN can be fatal if not rapidly treated.
- Community-onset urosepsis: Research shows lower mortality than some other sepsis sources, but outcomes hinge on timely, appropriate empiric therapy and local resistance patterns; MDR organisms markedly increase risk.
- Delayed care narratives: Multiple clinical summaries describe rapid escalation from flank pain and fever to ICU-level sepsis in 1–3 days without treatment, reinforcing that early intervention prevents the rare worst outcomes.
Table: Time course, risks, and outcomes
What to do at first symptoms
- Seek urgent medical assessment for fever with flank/back pain, nausea/vomiting, or urinary symptoms; do not wait, especially if older, diabetic, pregnant, or immunosuppressed.
- If symptoms include confusion, severe weakness, low blood pressure, fast breathing/heart rate, or very high fever, treat as an emergency and go to the ER due to sepsis risk.
- Expect urine testing, possible blood tests or imaging, and rapid initiation of antibiotics; source control (relieving obstruction) may be necessary.
Frequently Asked Questions (Q&A)
Q1: How quickly can a kidney infection become life-threatening?
A kidney infection can progress to urosepsis—and potentially fatal organ failure—within 24–72 hours if untreated or in high-risk individuals. Once sepsis is established, mean time to death is around 8 days, making rapid medical evaluation and antibiotics essential.
Q2: What symptoms signal that a kidney infection is worsening?
Warning signs include:
- High fever and chills
- Severe flank or back pain
- Confusion or altered mental status
- Rapid heartbeat (>90 bpm) or breathing (>20 breaths/min)
- Low blood pressure or dizziness
- Reduced urine output
These suggest sepsis and require immediate ER care.
Q3: Who is at greatest risk for rapid deterioration?
People aged over 65, those with diabetes, immunosuppression, urinary obstruction (stones, catheters), pregnancy, or recent urinary instrumentation face faster progression to severe sepsis and higher mortality.
Q4: Can antibiotics alone always prevent fatal outcomes?
Prompt, appropriate antibiotics usually halt progression; most patients improve within 48–72 hours. However, delays, resistant pathogens, or undrained obstructions can allow sepsis to develop, necessitating IV therapy, fluids, and sometimes surgical drainage.
Q5: How is a kidney infection diagnosed and treated?
Diagnosis relies on:
- Urine analysis and culture
- Blood tests (CBC, lactate, blood cultures)
- Imaging (ultrasound/CT) if obstruction or abscess is suspected
Treatment involves: - Oral or IV antibiotics
- IV fluids and supportive care for sepsis
- Relief of blockage via stenting or nephrostomy if needed.
Q6: What are the chances of recovery versus death?
In modern cohorts with rapid care:
- ~73% recover by 30 days
- ~19% have single organ failure
- ~5% have multiple organ failure
- ~3% die within 30 days of urosepsis diagnosis.
Q7: How can I reduce my risk of a severe kidney infection?
- Promptly treat lower UTIs with prescribed antibiotics
- Stay well-hydrated and fully empty your bladder
- Manage kidney stones and seek evaluation for recurrent UTIs
- Maintain catheter hygiene and remove indwelling devices promptly
- Discuss prophylaxis if you have recurrent infections or are at high risk.
Q8: When should I go to the emergency department?
Seek emergency care if you experience any of:
- Fever >38.9 °C (102 °F) with flank pain
- Confusion, fainting, or extreme weakness
- Rapid breathing or heartbeat
- Difficulty urinating or very low urine output
- Signs of shock (cold, clammy skin; severe dizziness).
Humanized perspective: balancing fear and facts
The phrase “how fast can a kidney infection kill you” reflects understandable fear, because the symptoms can escalate quickly and the stakes are high when sepsis develops. The reassuring truth is that most people recover with prompt antibiotics, and lasting harm or death is rare when care is not delayed. The uncomfortable truth is that for older adults or those with complicating factors, the window from “feeling sick” to “medical emergency” can be as short as a day or two, and that’s why acting early—rather than waiting—is the safest path.
Practical prevention
- Prevent lower UTIs: Hydration, bladder emptying, timely treatment of cystitis, and catheter care reduce risk of ascent to the kidney.
- Manage stones and obstructions: Address urolithiasis promptly and seek evaluation for recurrent UTIs or voiding issues to prevent blockages that trap infection.
- Know personal risk: Discuss prophylaxis or monitoring if pregnant, immunocompromised, or with recurrent UTIs; consider local resistance patterns for empiric choices.
External source notes
- Health system guidance emphasizes prompt evaluation and antibiotics for suspected pyelonephritis and flags life-threatening complications including sepsis, tissue damage, and death if severe and untreated.
- Patient-focused explanations clarify that while fatal outcomes are unlikely with timely care, kidney failure or sepsis can be catastrophic within days to weeks if not treated, reinforcing urgency.
- Specialty and academic literature quantify risk windows and mortality, showing that early antibiotics and source control underpin the favorable outcomes seen in modern cohorts.
References and external sources
- Cleveland Clinic Health Library: Kidney Infection (Pyelonephritis) — symptoms, complications, and treatment expectations.
- World Journal of Urology (2024): SERPENS multicenter study on urosepsis 30‑day mortality, morbidity, and risk factors; mean time to death 8.4 days; mortality 2.8% overall, 4.6% severe sepsis.
- Mayo Clinic: Kidney infection complications include blood poisoning (sepsis), tissue damage, and death; seek care promptly.
- Urology clinic overview: Sepsis can develop within 24–48 hours after severe symptoms if delayed care; vulnerable populations progress faster.
- Clinical explainer: Kidney infections can become dangerous within 24–72 hours in high-risk individuals; early antibiotics are protective.
- Large hospital cohort: Severe sepsis/septic shock in complicated pyelonephritis strongly increases 30‑day mortality; risk factors include age >65, instrumentation, and bacteremia.
- Patient-centered resources summarizing risks of untreated kidney infection, kidney failure, and sepsis timelines.
Medical Disclaimer
This article is intended for informational purposes only and does not constitute medical advice. The content provided is not a substitute for professional diagnosis, treatment, or care. Always consult a qualified healthcare provider with any questions regarding a medical condition or before beginning any treatment. Do not disregard professional medical advice or delay seeking it based on information in this article. If you believe you are experiencing a medical emergency, call emergency services or go to the nearest emergency department immediately.